Stroke is the second leading cause of mortality and the third leading cause of adult disability in the USA, causing severe long-term impairments in the lives of survivors. While the two kinds of stroke—ischaemic (85%) and haemorrhagic (15%)—differ in their origins, both culminate in compromised blood supply and subsequent brain ischaemia. This results in a critical shortage of oxygen necessary for cellular metabolic function and could potentially lead to lasting disability as neurons will begin to die after just a few minutes without oxygen. In this commentary, Shai Efrati and Amir Hadanny review the use of hyperbaric oxygen therapy (HBOT) for cognitive recovery after stroke.

Shai Efrati
Post-stroke impairment is common among stroke survivors and many experience physical dysfunction, (such as loss of voluntary motor skills or paralysis), speech difficulties, and/or cognitive dysfunction (such as memory loss, lack of attention or a decline in information processing speed). Traditional rehabilitation methods provide only partial relief and often leave the patient chronically disabled. The treatments largely focus on physical function but in general these have limited effects in which both motor and cognitive functions stabilise after approximately 30–90 days’ post stroke. After this period of time, recovery ceases and patients enter the “chronic late stage”, where after they are no longer expected to improve.
How HBOT affects the body and the brain
HBOT involves the inhalation of 100% oxygen at pressures exceeding 1 atmosphere absolute (ATA) in a pressurised chamber. HBOT is a well-established treatment for injuries such as serious infections, carbon monoxide toxicity, air bubbles in the blood vessels, and non-healing wounds resulting from diabetes or radiation burns.
Over the past decade, HBOT has been studied as a treatment for brain-related injuries or wounds, including traumatic brain injury, fibromyalgia and stroke. These studies have led to the new concept where the same components needed for recovery of non-healing wounds are also required for brain injuries, i.e. the non-healing brain “wounds”. The common denominator is the need to supply sufficient oxygen to the affected region (“the wound”) to enable tissue regeneration.
The second concept discovered was that the combined application of intermittent high oxygen concentration and pressure can induce a cascade of metabolic changes, cellular processes and events, which are usually triggered by a low level of oxygen (hypoxia) in the body. However, with HBOT treatment, the cascade is generated without the hazardous hypoxia, but rather by creating a high level of oxygen in the body, leading to regeneration (the hyperoxic-hypoxic paradox).
A generation of debate

Amir Hadanny
The idea that HBOT can provide a valuable tool for brain repair was first proposed almost half a century ago and has been considered anecdotal ever since. Interest was renewed in the mid-1990s, but the results were either ignored or questioned by the medical community. This was until Huang and Obenaus published a review in 2011, in which they presented an objective summary of the clinical trials, associated debate, and a thoughtful description of the animal studies and their implications.
The relatively new scientific insights on the physiological effects of the hyperoxic-hypoxic paradox, initiated an ongoing research programme, which takes a comprehensive and innovative approach to brain injuries. Cumulative evidence from both post-stroke and traumatic brain injury studies demonstrate that HBOT can induce neuroplasticity, the recovery of damaged brain tissue, in the chronic metabolic dysfunctional brain regions even years after the insult. The metabolic dysfunction brain regions can be identified by the use of the novel brain imaging modalities. This has led to the understanding that imaging-based patient selection is crucial and may explain previous studies’ failure.
How HBOT can improve the effects of stroke
A stroke can often leave a person with two degrees of brain injuries. The most severe is necrosis, fully dead tissue, which cannot be recovered with HBOT. However, in some areas, the insult may be less severe, and a chronic penumbra, or “stunned” brain tissue is formed. The penumbra is characterised by cells with metabolic dysfunction, which have the minimal energy needed to survive but cannot generate the energy required for normal brain function. The penumbra usually surrounds the initial core of the necrotic tissue, and this stagnated state can persist for years.
While the decreased cellular oxygen metabolism observed after a stroke causes reduced neuronal activity and prevents recovery, HBOT’s novel hyperoxygenation enables the generation of new synaptic connections and angiogenesis (generation of new blood vessels), improves mitochondrial function, improves cerebral metabolism, reduces inflammation and effects beyond-synaptic changes, such as regenerating axonal white matter, stimulating axonal growth, and promoting blood-brain barrier integrity. In short, by improving oxygenation of these “border zones” of necrotic tissue, we can rejuvenate neurons that were previously deemed non-functional.
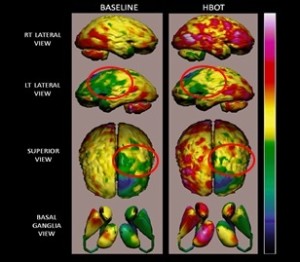
Figure 1
For stroke patients in particular, if selected appropriately, HBOT has been proven to induce neuroplasticity even years after the acute stroke. The clinical improvement will be directly correlated with the dysfunctional brain tissue revealed using brain imaging. For example, the brain imaging of a 72-year-old man who had hemiparesis related to ischaemic stroke, which occurred 34 months prior to him starting HBOT, showed in a baseline examination a lack of strength to hold the right leg and hand against gravity. He also had moderate aphasia. After treatment he had significant improvement in the motor function of both hand and leg with increased strength to hold them both against gravity. He also experienced significant improvement in his fine motor skills. Language communication was significantly improved and he regained the ability to complete sentences—a major improvement to his quality of life. Correlated with the physical function, brain imaging demonstrated significant metabolic increase in the areas which control both motor and speech functions.
New hope for recovery
New trials provide convincing evidence that HBOT can, in fact, induce neuroplasticity, leading to repair of chronically impaired brain function and improved quality of life in post-stroke patients even years after the initial insult—as long there is metabolic dysfunction.
As with any treatment, there are risks associated with the administration of HBOT if not done appropriately, and this treatment must be administered using the tested protocols with the correct medical supervision. While there is still much research to be done on this neurotherapeutic method for brain injury repair, hyperbaric oxygen treatment may be a long-awaited treatment option for cognitive recovery after stroke.
Shai Efrati is the founder and director of the Sagol Center for Hyperbaric Medicine and Research at Shamir Medical Center, Be’er Ya’akov, Israel.
Amir Hadanny is the chief medical research officer at the Sagol Center for Hyperbaric Medicine and Research, Shamir Medical Center, Be’er Ya’akov, Israel